
- Laboratory of Molecular Biology, Fundación Instituto Valenciano de Oncología, Valencia, Spain
- Department of Medical Oncology, Fundación Instituto Valenciano de Oncología, Valencia, Spain
- Department of Medical Oncology, Hospital Arnau de Villanova, Lleida, Spain
- Department of Pathology, Fundación Instituto Valenciano de Oncología, Valencia, Spain
- Department of Pathology, University of Valencia, Spain
- Department of Radiology, Fundación Instituto Valenciano de Oncología, Valencia, Spain
- Department of Surgery, Fundación Instituto Valenciano de Oncología, Valencia, Spain
Received: 3 September 2009
Accepted: 9 February 2010
Published: 9 February 2010
© 2010 Garcia-Casado et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Aromatase (CYP19A1) regulates estrogen biosynthesis. Polymorphisms in CYP19A1 have been related to the pathogenesis of breast cancer (BC). Inhibition of aromatase with letrozole constitutes the best option for treating estrogen-dependent BC in postmenopausal women. We evaluate a series of polymorphisms of CYP19A1 and their effect on response to neoadjuvant letrozole in early BC.
We analyzed 95 consecutive postmenopausal women with stage II-III ER/PgR [+] BC treated with neoadjuvant letrozole. Response to treatment was measured by radiology at 4th month by World Health Organization (WHO) criteria. Three polymorphisms of CYP19A1, one in exon 7 (rs700519) and two in the 3'-UTR region (rs10046 and rs4646) were evaluated on DNA obtained from peripheral blood.
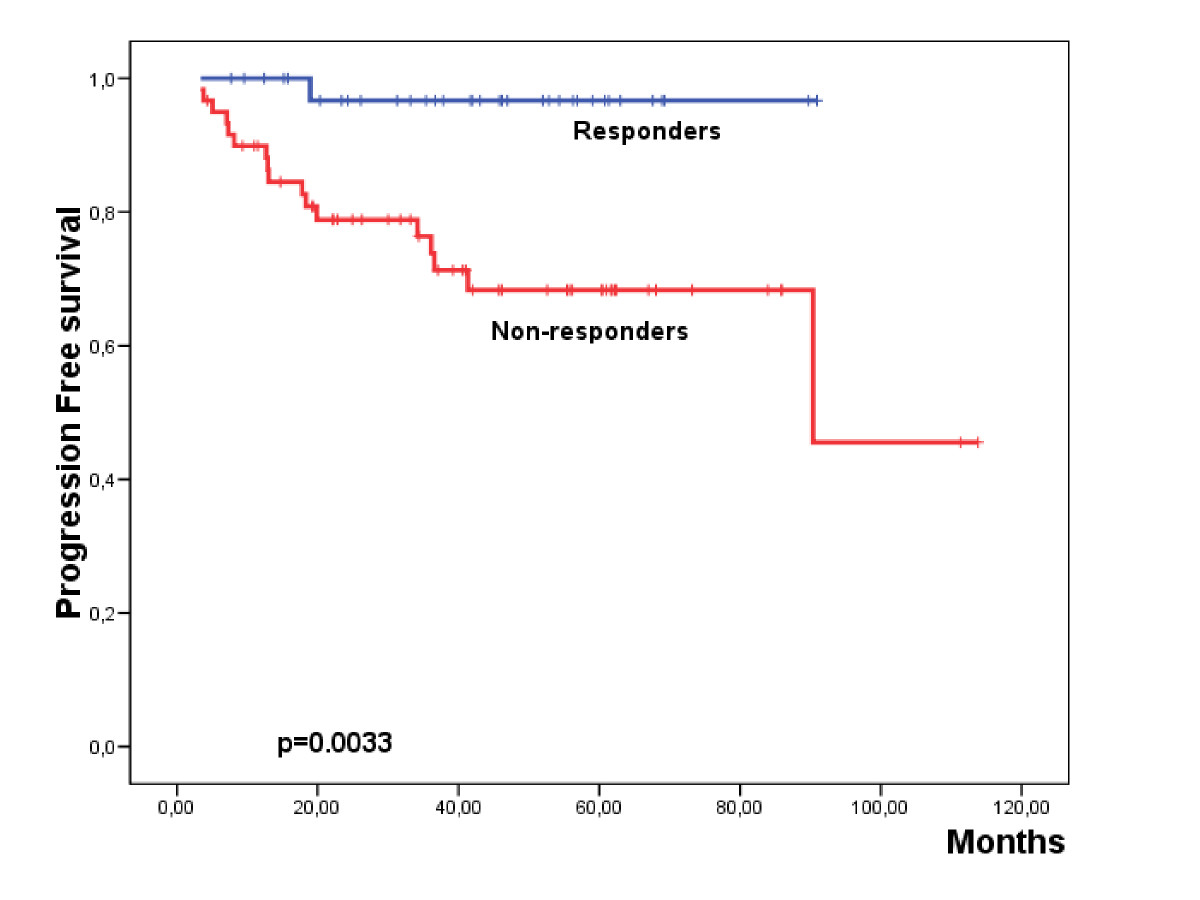
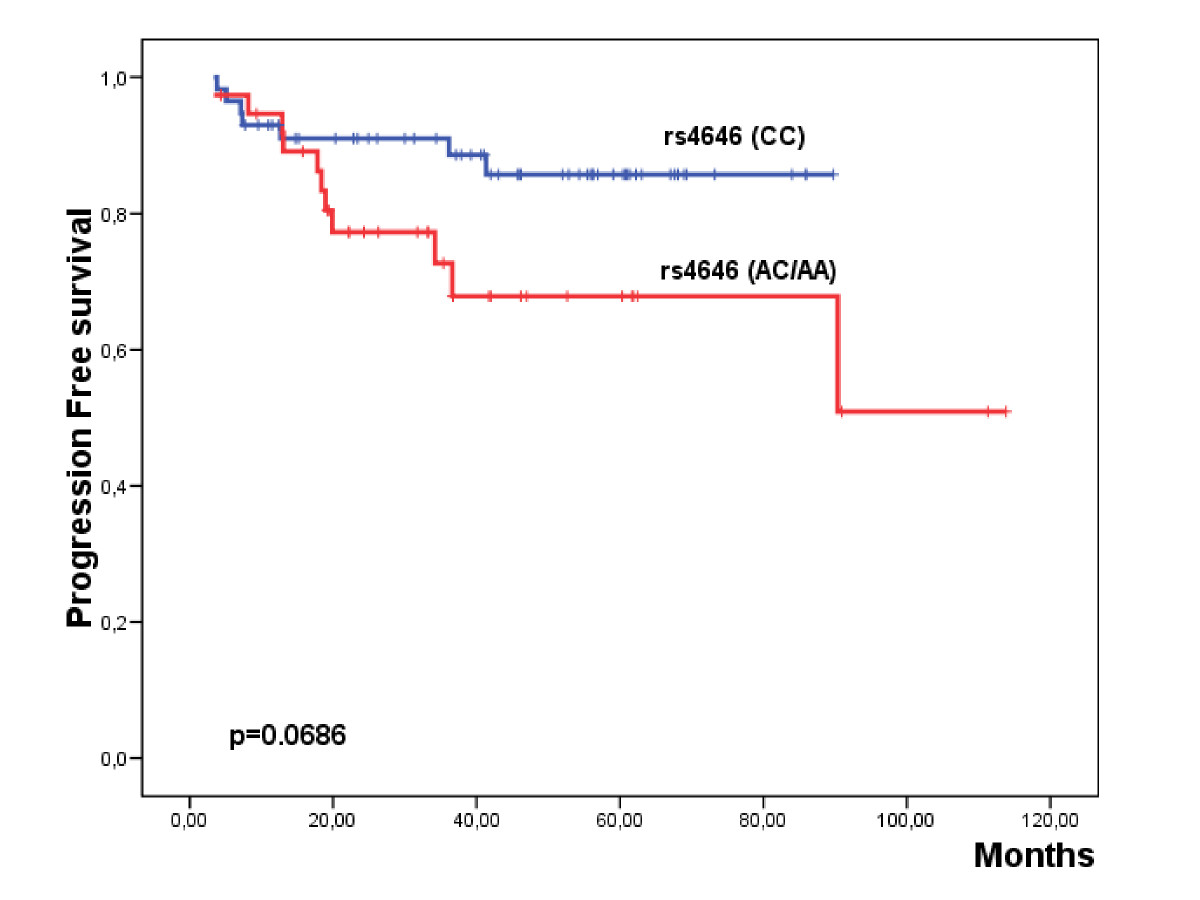
Thirty-five women (36.8%) achieved a radiological response to letrozole. The histopathological and immunohistochemical parameters, including hormonal receptor status, were not associated with the response to letrozole. Only the genetic variants (AC/AA) of the rs4646 polymorphism were associated with poor response to letrozole (p = 0.03). Eighteen patients (18.9%) reported a progression of the disease. Those patients carrying the genetic variants (AC/AA) of rs4646 presented a lower progression-free survival than the patients homozygous for the reference variant (p = 0.0686). This effect was especially significant in the group of elderly patients not operated after letrozole induction (p = 0.009).
Our study reveals that the rs4646 polymorphism identifies a subgroup of stage II-III ER/PgR [+] BC patients with poor response to neoadjuvant letrozole and poor prognosis. Testing for the rs4646 polymorphism could be a useful tool in order to orientate the treatment in elderly BC patients.
After cessation of ovarian activity at postmenopause, the aromatase [cytochrome P450 19 (CYP19); OMIM:107910] from bones, adipose tissue and muscle, becomes the key enzyme in estradiol and estrone biosynthesis through the aromatization of testosterone and androstenedione respectively(1). Aromatase is encoded by CYP19A1 which maps at chromosome 15q21.1 and has a complex structure with a region that contains 10 tissue-specific non-coding upstream exons with separate promoters that regulate transcription in different cells and tissues(2). Elevated levels of aromatase expression have been observed in breast tumors relative to normal breast tissue(3), and alterations in aromatase expression have been implicated in the pathogenesis of estrogen-dependent diseases, including breast cancer (BC)(4)(5).
The major biological characteristic of BC is that two thirds of cases express estrogen (ER) and/or progesterone receptors (PgR)(2)(6)(7), endocrine manipulation being an effective treatment for these patients. Tamoxifen, a selective ER modulator, has for decades been the gold standard therapy in ER/PgR [+] BC patients(8). However, in postmenopausal patients, aromatase inhibitors like letrozole have consistently demonstrated to be more effective than tamoxifen(9). Letrozole is highly specific for the aromatase enzyme and inhibits whole-body aromatization of almost 99%, providing a highly and essentially complete withdrawal of estrogen in postmenopausal women(10).
Neoadjuvant hormonal therapy is a safety option for postmenopausal women with large operable or locally advanced hormone sensitive BC, increasing the possibilities of breast-conserving surgery (BCS)(11). In this context, letrozole has shown to be more effective than tamoxifen, obtaining higher response and BCS rates following 4 months of preoperative therapy(12)(13). However, less than 60% of patients will respond to this optimal endocrine therapy(14). To date, only the presence and intensity of hormonal receptors (ER/PgR) are useful tools as predictive markers in clinical practice. Identification of more accurate markers for more efficient patient selection to exclude non-responsive cases remains crucial.
Genetic polymorphisms in the CYP19A1 gene have been associated with altered sex hormone levels in serum and urine(15)(16)(17), providing an explanation for an elevated risk for BC in relation to estrogen exposure. For example, the tetranucleotide repeat polymorphism in intron 4 (TTTA)n has been associated with BC risk in initial studies(18)(21)(22). The polymorphism rs10046 in the 3' untranslated region (3'-UTR) also showed inconsistent associations with BC risk(23)(24)(25)(26) and has also been related with tumor stage(25), circulating sex hormone levels(15), HER2 status and disease free and overall survival(27)(28). rs4646 has been reported to be associated with circulating steroid hormone levels(17) and, as in rs10046, with the HER2 status of the tumor(27). Hence, it is biologically plausible that the polymorphisms in the CYP19A1 gene may be associated with the response to aromatase inhibitors. Indeed, recently the rs4646 CYP19A1 polymorphism has been associated with letrozole efficacy in advance disease(29); however, no evidence between CYP19A1 polymorphisms and therapeutic efficacy of aromatase inhibitors in early stage BC has yet been established.
In the present study, we perform a genetic analysis of three CYP19A1 polymorphisms in a series of postmenopausal endocrine-sensitive BC patients treated with neoadjuvant letrozole and describe their association both with radiological response at 4 months (RR4M) of treatment and with progression free survival (PFS).
Finally, 95 patients fulfilled all criteria, were contacted by their physician (AGZ, ALC, ARS, JG, MAC, VG) and agreed to participate on the study. All patients gave their written consent for the use of their DNA for this specific research proposal. In addition, this study was reviewed and approved by the FIVO Science and Ethics Committees.
Peripheral blood samples (7 ml) were obtained from these patients and processed for DNA extraction at the Laboratory of Molecular Biology.
Response to treatment at four months was done using the WHO criteria: complete response (CR) required the complete disappearance of all disease, partial response (PR) was defined as a reduction of ≥ 50% in tumor volume and stable disease (SD) was any reduction < 50% in tumor volume. The response evaluation was done by an independent radiologist (JCD).
Pre-treatment study included patient characteristics, menopausal status, disease history, histological grade and diagnosis, evaluation of hormone receptor status, HER2 and Ki67 status by immunohistochemical analysis on core-cut biopsies, ECOG performance status and tumor assessment. The clinical data were prospectively reviewed and stored within a specific database.
Four-micrometer sections from embedded blocks were cut on poly-L-lysine-coated slides, and dewaxed, endogenous peroxidase was inhibited with 3% hydrogen peroxide for 30 min. Immunoreactivity was enhanced with antigen retrieval treatment by heating the slides in a microwave oven for 10 min (700 W) in 10 mM sodium citrate buffer pH 7, followed by cooling for 20 min at room temperature. Sections were blocked with 20% horse serum in phosphate-buffer saline (PBS) and incubated with primary antibody for 1 h at room temperature. The incubation time for the secondary antibody and avidin-biotin complexes was 30 min at room temperature. Sections were extensively washed and the immunoreactions developed using DAB (0.05% 3'3' diamino-benzidine in 0.1% hydrogen peroxide). Negative controls included substitution of the primary antibody by mouse ascites or PBS. Slides were counterstained in Mayer hematoxylin, dehydrated, and mounted.
ER and PgR expression in primary tumor was immunohistochemically evaluated using the anti-ER (clone 6F11) and anti-PgR (clone 1A6) antibodies (Novocastra Laboratories, Newcastle upon Tyne, England) at a dilution of 1:40 and 1:30 respectively. Ki67 expression was also determined using the anti-Ki67 (clone MIB1) antibody (Dako Corp., Carpinteria, CA) at a 1:50 dilution.
HER2 protein expression was immunohistochemically evaluated using the HercepTest Kit (Dako Corp., Carpinteria, CA) according to the manufacturer's protocol. The scoring system was as follows: 0, tumors with no or weak staining in less than 10% of the cells; +, tumors with a faint or barely perceptible membrane staining in more than 10% of cells or with noncircumferential staining; ++, moderate circumferential membrane staining; +++, strong circumferential membrane staining. Scores 0 and + were considered as negative; scores ++ and +++ were considered as positive for HER2 overexpression(31).
Genotyping of the rs10046 and rs4646 polymorphisms were carried out by allelic discrimination using specific TaqMan SNP Genotyping Assays and following the manufacturer's instructions. In brief, 20 μl PCR reactions were carried out containing 10.0 μl TaqMan Universal PCR Master Mix (Applied Biosystems, New Jersey, USA), 20.0 ng DNA template and 1.0 μL TaqMan SNP Genotyping Assays (Applied Biosystems, Foster City CA 94404). The references of selected assays were: C_8234731_1 (rs10046) and C_8234730_1 (rs4646). All assays were performed in 96-well plates including non-template controls. PCR reactions were read on a 7500 Fast Real Time PCR System in end-point mode using the Allelic Discrimination Sequence Detector software (Applied Biosystems).
For the statistical analysis we used binary variables reflecting the positivity status of the measures (yes or no) as well as the genotypic status of each polymorphism (homozygous reference or heterozygous/homozygous less frequent). Association with histopathological parameters, all categorical, was also assessed using a chi-square test to determine homogeneity or linear trend for ordinal variables. The significance level was set at 5%.
Deviations of genotype frequencies from those expected under Hardy-Weinberg equilibrium (HWE) were assessed by χ2 (p > 0.05) tests(33).
To study the impact of the biological factors on progression-free survival (PFS), the Kaplan-Meier proportional risk test (Log Rank) was used(34)(35). PFS was defined as the time interval from the start of treatment to local or distant disease progression. Those patients that reported disease progression during the follow-up were considered as censored, being the data of confirmation of this progression considered in the calculation of PFS. Univariate predictors of PFS were entered into a Cox proportional hazards model using stepwise selection to identify the independent predictors of poor outcome, a confidence interval (CI) of 95% was also considered(36).
| Parameter |
n (%) |
|---|---|
|
|
|
| Histological diagnosis* |
|
| IDC |
67 (70.5) |
| ILC |
16 (16.8) |
| Others |
12 (12.6) |
| Histological grade |
|
| I |
29 (55.8) |
| II |
19 (36.5) |
| III |
4 (7.7) |
| Tumor size (T) |
|
| T2 |
76 (80.0) |
| T3-T4 |
19 (20.0) |
| Lymph node involvement (N) |
|
| N0 |
76 (80.0) |
| N1-2 |
19 (20.0) |
| Stage |
|
| IIa |
65 (68.4) |
| IIb |
20 (21.1) |
| IIIa-IIIb |
10 (10.5) |
| ER |
|
| Negative |
5 (5.3) |
| 10-40% |
8 (8.4) |
| 40-70% |
25 (26.3) |
| > 70% |
57 (60.0) |
| PgR |
|
| Negative |
28 (29.5) |
| 10-40% |
18 (18.9) |
| 40-70% |
24 (25.3) |
| > 70% |
25 (26.3) |
| HR** |
|
| ≤ 40% |
10 (10.5) |
| > 40% |
85 (89.5) |
| HER2 |
|
| Negative |
39 (41.1) |
| + |
24 (25.3) |
| ++ |
22 (23.2) |
| +++ |
10 (10.5) |
| Ki67 |
|
| Negative |
40 (55.6) |
| Positive |
32 (44.4) |
| Response to letrozole |
|
| Non responders |
60 (63.2) |
| Responders |
35 (36.8) |
| Progression status |
|
| No progression |
77 (81.1) |
| Progression |
18 (18.9) |
| Surgery status |
|
| No surgery |
30 (32.0) |
| Surgery |
65 (68.0) |
*IDC, Infiltrating ductal carcinoma; ILC, Infiltrating lobular carcinoma; Others (Mucinous, tubular and medullar carcinomas).
**Hormonal status was considered as ≤ 40% when either estrogen and progesterone receptors were ≤ 40%, and as > 40% when at least one of the receptors were > 40%.
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
The median treatment period with letrozole as neoadjuvant therapy was 10.23 months (range: 3.53-85). Response to treatment was evaluated by radiological means (mammogram or ultrasound) at four months of letrozole administration using WHO criteria(37). A total of 34 partial responses (PR) and one complete response (CR) where achieved, and were classified as responders for the analysis. Hence, the overall radiological response rate at 4 months (RR4M) was 36.8%. On the contrary, 55 women remained with stable disease (SD) and 5 developed progression disease (PD), these all being considered as non-responders.
| db-SNP id |
Genotype |
n (%) |
p* |
Gene location |
Chromosome position** |
|---|---|---|---|---|---|
|
|
|||||
| rs700519 |
CC |
89 (100) |
- |
Exon 7 (codon 264) |
49.295.260 |
| CT |
0 (0) |
||||
| TT |
0 (0) |
||||
| rs10046 |
AA |
23 (24.2) |
0.127 |
3'UTR |
49.290.278 |
| AG |
57 (60.0) |
||||
| GG |
15 (15.8) |
||||
| rs4646 |
CC |
57 (60.0) |
0.397 |
3'UTR |
49.290.136 |
| AC |
30 (31.6) |
||||
| AA |
8 (8.4) |
||||
*p > 0.05 is consistent with the Hardy-Weinberg equilibrium; ** Sequence of reference NT_010194.16.
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
| Parameters |
Responders (%) |
Non-responders (%) |
p |
|---|---|---|---|
|
|
|||
| Age (years) |
|||
| ≤ 78.3 |
19 (54.3) |
29 (48.3) |
0.576 |
| > 78.3 |
16 (45.7) |
31 (51.7) |
|
| Histological diagnosis |
|||
| IDC |
25 (71.4) |
42 (70.0) |
0.843 |
| ILC |
5 (14.3) |
11 (18.3) |
|
| Others |
5 (14.3) |
7 (7.4) |
|
| Histological grade |
|||
| I |
13 (61.9) |
16 (51.6) |
0.606 |
| II |
6 (28.6) |
13 (41.9) |
|
| III |
2 (9.5) |
2 (6.5) |
|
| Tumor size (T) |
|||
| T2 |
31 (88.6) |
45 (75.0) |
0.111 |
| T3-T4 |
4 (11.4) |
15 (25.0) |
|
| Lymph node involvement (N) |
|||
| NO |
28 (80.0) |
48 (80.0) |
1.000 |
| N1-2 |
7 (20.0) |
12 (20.0) |
|
| Stage |
0.546 |
||
| IIa |
26 (74.3) |
39 (65.5) |
|
| IIb |
7 (20.0) |
13 (21.7) |
|
| IIIa-IIIb |
2 (5.7) |
8 (13.3) |
|
| ER |
|||
| ≤ 40% |
3 (8.6) |
10 (16.7) |
0.268 |
| > 40% |
32 (91.4) |
50 (83.3) |
|
| PgR |
|||
| ≤ 40% |
15 (42.9) |
31 (51.7) |
0.407 |
| > 40% |
20 (57.1) |
29 (48.3) |
|
| HR |
|||
| ≤ 40% |
2 (5.7) |
8 (13.3) |
0.243 |
| > 40% |
33 (94.3) |
52 (86.7) |
|
| HER2 |
|||
| 0, + |
21 (60.0) |
42 (70.0) |
0.320 |
| ++, +++ |
14 (40.0) |
18 (30.0) |
|
| Ki67 |
|||
| Negative |
15 (55.6) |
25 (55.6) |
1.000 |
| Positive |
12 (44.4) |
20 (44.4) |
|
| rs10046 |
|||
| GG |
6 (17.1) |
9 (15.0) |
0.782 |
| AG/AA |
29 (82.9) |
15 (85.0) |
|
| rs4646 |
|||
| CC |
26 (74.3) |
31 (51.7) |
0.030 |
| AC/AA |
9 (25.7) |
29 (48.3) |
|
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
Format: DOC Size: 38KB Download file
This file can be viewed with: Microsoft Word Viewer
This table shows the associations of the clinicopathological and genetic parameters with PFS that have not been statistically significant.
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
Click image to view larger.
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
Click image to view larger.
| Parameters |
n |
Events |
%PFS |
p |
|---|---|---|---|---|
|
|
||||
| Tumor size |
||||
| T2 |
76 |
12 |
62.6 |
0.089 |
| T3-T4 |
19 |
6 |
59.3 |
|
| Lymph node involvement |
||||
| N0 |
76 |
10 |
57.31 |
0.0011 |
| N1-N2 |
19 |
8 |
44.7 |
|
| Stage |
||||
| IIa |
65 |
8 |
58.2 |
0.0232 |
| IIb |
20 |
6 |
65.1 |
|
| IIIa-IIIb |
10 |
4 |
42.3 |
|
| RR4M |
||||
| Responders |
35 |
1 |
96.7 |
0.0033 |
| Non-responders |
60 |
17 |
45.6 |
|
| rs10046 |
||||
| GG |
18 |
3 |
80.0 |
0.967 |
| AG/AA |
80 |
15 |
81.3 |
|
| rs4646 |
||||
| CC |
57 |
7 |
85.7 |
0.0686 |
| AC/AA |
38 |
11 |
50.9 |
|
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
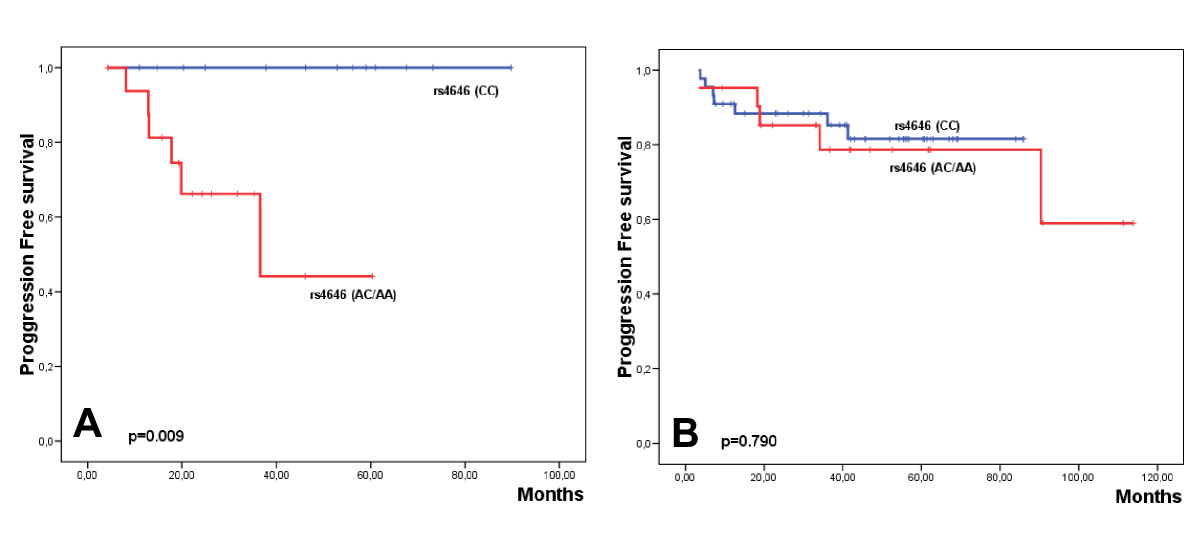
Univariate analysis performed for PFS for each group of patients revealed that in the non-surgery group, RR4M and r4646 where associated with a worse prognosis (Table 5; Additional file 2: Supplemental Table S2). Indeed, the 6 patients who progressed were genetically characterized by the variant rs4646 (AC/AA) (Fig. 3A). However, in the multivariate analysis only the polymorphism rs4646 emerged as an independent prognostic factor although it did not reach statistical significance (p = 0.191).
Format: DOC Size: 55KB Download file
This file can be viewed with: Microsoft Word Viewer
This table shows the associations of the clinicopathological and genetic parameters with PFS that have not been statistically significant according to surgery status.
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
Click image to view larger.
| No surgery |
Surgery |
|||||||
|---|---|---|---|---|---|---|---|---|
|
|
||||||||
| Parameters |
n |
Events |
%PFS |
p |
n |
Events |
%PFS |
p |
| Ki67 |
||||||||
| Negative |
17 |
5 |
66.9 |
0.686 |
23 |
1 |
50.0 |
0.023 |
| Positive |
5 |
1 |
80.0 |
27 |
8 |
69.6 |
||
| RR4M |
||||||||
| Responders |
10 |
0 |
100 |
0.041 |
25 |
1 |
95.2 |
0.030 |
| Non-responders |
20 |
6 |
58.8 |
40 |
11 |
47.8 |
||
| rs4646 |
||||||||
| CC |
13 |
0 |
100 |
0.009 |
44 |
7 |
81.5 |
0.790 |
| AC/AA |
17 |
6 |
44.1 |
21 |
5 |
59.0 |
||
Garcia-Casado et al. BMC Cancer 2010 10:36 doi:10.1186/1471-2407-10-36
In the group of patients operated after letrozole induction, only Ki67 expression and RR4M were associated with worse PFS (Table 5; Additional file 2: Supplemental Table S2), although none of these variables were independent indicators of poor outcome. Contrary to that observed in the non-surgery group, no association of the rs4646 variants with PFS was observed (Fig. 3B).
We describe a relationship between the genetic variants (AC/AA) of the rs4646 polymorphism of CYP19A1 and a poor response to neoadjuvant treatment with letrozole in postmenopausal women with ER/PgR [+] BC. The radiological response was measured at the 4th month of letrozole induction, the observed response rate being 36.8%, similar to the radiological response reported in the P024 trial(12).
At genetic level, mutations in the aromatase gene may lead to a functionally less sensitive aromatase phenotype. Although mutations in the CYP19A1 gene can be generated in vitro, to date no somatic mutation has been found in clinical samples (38). However, several genetic polymorphisms of CYP19A1 have been reported so far, although the possible functional significance of most of these remains undefined. In the case of BC, population-based studies of common CYP19A1 polymorphisms have generated inconsistent results with regard to their possible association with sex hormone levels, cancer risk, HER2 status or survival [15,19,21,27,28]. No association between the HER2 or hormonal status of either rs10046 or rs4646 was observed in our series.
Whether aromatase inhibitor agents interact with the different CY19A1 genotypes has not so far been clearly established. Only three previous studies have attempted to demonstrate the effect of certain polymorphisms in CYP19A1 on the efficacy of aromatase inhibitors. In the first, Fasching et al., in a series of patients treated with hormonal therapy for more than 2 years, did not observe significant differences between the rs700519, rs10046 and rs4646 polymorphisms with therapy. Unfortunately, the type of antihormonal therapy was not recorded for this analysis(27). In the second study, a population-based and in vitro study, Ma et al. revealed reductions in the functional activity of aromatase for four phenotypes resulting from non-synonymous changes [rs700519 (Arg264Cys), rs28757184 (Thr201Met), rs2236722 (Trp39Arg), and rs56658716 (Met364Thr)](32). These authors found that levels or aromatase enzyme activity decreased dramatically for the Thr364, and also observed a slight decrease in Cys264 allozyme activity. They also demonstrated that the mechanism by which non-synonymous SNPs affect the enzymatic activity is a consequence of an alteration in the enzyme protein level(32). In the same study, these authors reported that these variants had no significant differences in their affinity to the aromatase inhibitors letrozole and exemestane(32). Interestingly, the polymorphism rs700519 has also been reported as a prognostic factor in a Chinese study, mainly in a subgroup of premenopausal women(28), but not in the Caucasian population(27). In addition, it is important to note the differences between these two populations regarding the minor allele frequency of rs700519, being only 3.2% for the Caucasian population (1,257 patients)(27), in comparison with 15.1% in the Asian Cohort (1,136 patients)(28). In our series, the genetic variants of this polymorphism were underrepresented and not found in any of the cases.
The third study evaluated the efficacy of treatment with letrozole in advanced hormone receptor-positive BC patients with respect to two polymorphisms located at the 3'-UTR (rs10046 and rs4646) and one in intron 2 [rs727479 (G/T)] of the CYP19A1(29). The authors found that genetic variants of rs4646 were associated with a greater efficacy of letrozole in terms of time to progression. Hence, patients with the variant genotype (AC/AA) had a three times greater time to progression than the patients with the reference genotype (CC). Furthermore, these authors reported that the frequency of the variant alleles for rs4646 was significantly higher in the responder (61%) than in the non-responder group of patients (40%)(29). These observations clearly differ from those reported in our series, the genotypic variants of rs4646 being more frequently represented in the non-responder group to letrozole after 4 months of induction therapy (48% vs. 26%). In this regard, there are two main issues that could explain the differences between these two studies. First, and independently of the disease stage, are the criteria for patient selection. Whereas in our series the patients were treated with letrozole as a first line, in the study of Colomer et al. the patients had progressed from a previous treatment with tamoxifen(29). It is well established that tamoxifen metabolism is influenced by the number of mutant alleles of the gene encoding cytochrome P450 2D6 (CYP2D6), because this enzyme affects the levels of endoxifen, the active tamoxifen metabolite. Thus, for patients who are wild type for CYP2D6, the 5-year disease-free survival outcomes are similar to or perhaps even superior with tamoxifen than with aromatase inhibitors(39). Therefore, previous treatment with tamoxifen could have genetically selected a population of patients more sensitive to letrozole. Secondly, in our study we used constitutive DNA obtained from peripheral blood for the genetic analysis, whereas Colomer et al. performed the genetic study on DNA obtained from the fixed and paraffin-embedded tumors(29). The polymorphism studies performed on tumor samples are subject to genetic alterations that can affect the chromosomal region of the gene under study. In this way, CYP19A1 is located in the 21.2 region of the long arm of chromosome 15 (15q21.2)(40), and this region has been reported to be a frequent target of allelic imbalance in advanced breast carcinomas(41), and which could affect the frequency distribution of the allelic variants.
From our series, 65 women underwent surgery after letrozole induction, being age the only difference observed between the operated and non-operated patients. In fact 77% of patients within the non-surgery group were over 78.3 years. We have demonstrated that genetic variants of rs4646 have prognostic value, especially in this group of patients. Indeed, the 6 women who progressed within the group of non-surgery patients were genetically characterized by the variant rs4646 (AC/AA). In this elderly group of patients the decision for undergoing surgery is not always easy and very often both the patient and the clinician opt for a local control of the tumor maintaining the treatment with letrozole. Hence, in this group of patients, in which the tumor is not removed, is where the rs4646 polymorphism identifies the women who progressed, indicating, and despite the small number the cases included in our series, that women with the rs4646 (AC/AA) genotype could benefit from another therapeutic approach.
The regulatory interactions between the ER, growth factor receptors and other kinase signalling pathways could also determine the response to endocrine therapy. In the adjuvant setting, several studies suggest that patients overexpressing HER2 may derive relatively less benefit from endocrine therapy(38). In the P024 trial, ER [+] tumors that were also EGFR and/or HER2 [+] responded significantly better to letrozole than to tamoxifen (88% vs 21% respectively, P = 0.0004)(13). The IMPACT study, that confronted tamoxifen with anastrozole, or the preoperative combination of both, observed a similar effect in favour of anastrozole for HER2 [+] tumors (Odds Ratio 58% vs. 22%), although not reaching statistical significance(42). In our series, as in both randomized trials, no differences in activity were observed relating to HER2 expression among the patients receiving letrozole.
Biological studies of tissues obtained during neoadjuvant therapy have thrown a different perspective on this issue. Short-term estrogen deprivation leads to profound changes in transcriptional profiles, and these changes can be used as predictive tools. Tumor expression of the proliferation antigen Ki67 after 2 weeks of endocrine treatment (tamoxifen or anastrozole) predicts for clinical response and recurrence-free survival(42). However, among cases on anastrozole, only 7% did not present a reduction in the Ki67 expression at 2 weeks. In many cases, this reduction in the tumor proliferation rate is only modest and could not be sufficient to determine a resistance to the treatment. As expected, early tumor changes are not limited to proliferation markers, but to other genes directly regulated by ER, including the aromatase itself(43). Other, currently ongoing, approaches have used gene expression profiling techniques able to predict response to endocrine therapy, but the results obtained so far are inconsistent(43). In our series, expression of proliferating marker Ki67 constituted a factor of poor prognosis in the group of patients undergoing surgery following letrozole induction therapy, suggesting that this marker could identify tumors with a more aggressive behavior.
We have found that genetic variants of the polymorphism rs4646 in the 3'-UTR of CYP19A1 are associated to poor response to letrozole after 4 months induction therapy and to poor outcome of elderly patients without surgery after letrozole administration in postmenopausal women with ER/PgR [+] BC. Although our study would suggest that analysis of rs4646 could improve the clinical management of these patients by facilitating a more individualized therapy, further studies based on larger series are necessary to confirm these findings.
3'-UTR: 3'-untranslated region; CYP19A1: aromatase gene; BC: breast cancer; BCS: breast conserving surgery; CR: complete response; DAB: diamino-benzidine; ER: estrogen recetor; HWE: Hardy-Weinberg equilibrium; IDC: infiltrating ductal carcinoma; ILC: infiltrating lobular carcinoma; PR: partial response; PBS: phosphate-buffer saline; PgR: progesterone receptor; PD: progression disease; PFS: progression free survival; RR4M: radiological response at 4 months; SNPs: single nucleotide polymorphisms; SD: stable disease; WHO: World Health Organization.
The authors declare that they have no competing interests.
ZGC carried out the molecular genetic studies, participated in the genetic analysis and drafted the manuscript. AGZ reviewed the clinical records of the patients included in the study and drafted the manuscript. AFS performed the genetic analysis. ALlC, ARS, JG, MAC and VG treated most of the patients included in the study and updated the clinical follow-up. AC, SA and ALlB carried out the histopathological and immunohistochemical analysis. JCD performed the radiological evaluation of the study. JC and CVA performed the trucut biopsies and informed to the patients about the study. JALG conceived of the study, performed the statistical analysis and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
We thank Maria Garcia Flores, Tania Mazcuñan and Laura Martinez for their technical assistance.
This study has been financed by grants GV0A6/256 from the Conselleria d'Empresa Universitat i Ciència of the Generalitat Valenciana (JALG) and SOLTI 06/01 (ALLC).
The pre-publication history for this paper can be accessed here:
http://www.biomedcentral.com/1471-2407/10/36/prepub
