
- Department of Pediatric and Adolescent Oncology, Gustave Roussy Institute, 39 Rue Camille Desmoulins, 94805 Villejuif, France
- Department of Radiation Therapy, Gustave Roussy Institute, Villejuif, France
- LIMEC, INSERM UMR 788, University Hospital, Kremlin-Bicêtre, France
- Centre de Protonthérapie, Orsay, France
- Department of Neuropathology, Sainte-Anne Hospital, Paris, France
- Depatment of Neurosurgery, Necker Sick Children's Hospital, Paris, France
Radiation Oncology 2010, 5:9 doi:10.1186/1748-717X-5-9
Received: 15 October 2009
Accepted: 4 February 2010
Published: 4 February 2010
© 2010 Meyzer et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A fourteen years-old boy was treated post-operatively with proton therapy for a recurrent low-grade oligodendroglioma located in the tectal region. Six months after the end of irradiation (RT), a new enhancing lesion appeared within the radiation fields. To differentiate disease progression from radiation-induced changes, dynamic susceptibility contrast-enhanced (DSCE) MRI was used with a T2* sequence to study perfusion and permeability characteristics simultaneously. Typically, the lesion showed hypoperfusion and hyperpermeability compared to the controlateral normal brain. Without additional treatment but a short course of steroids, the image disappeared over a six months period allowing us to conclude for a pseudo-progression. The patient is alive in complete remission more than 2 years post-RT.
The occurrence of new contrast enhancing lesions on routine MRI follow-up after radiation therapy (RT) for brain gliomas was observed more than ten years ago but remains problematic because standard MR imaging techniques do not allow a clear distinction between recurrent tumour and radiation-induced lesions(1)(2). Recently, "pseudo-progression" was defined as conventional MR images compatible with progression, occurring shortly after concomitant radio-chemotherapy (CRC), as a transient phenomenon with spontaneous improvement or stabilization after several months(3)(4)(5). This was mainly described in adult and paediatric populations with high-grade gliomas whose new standard of care is CRC followed by adjuvant chemotherapy(6)(7).
We report here a clinical case showing a new contrast-enhancing lesion discovered on a systematic MRI proposed to a fourteen years-old boy treated six months before for a recurrent low-grade glioma by surgery and proton-therapy. Dynamic Susceptibility Contrast (DSC) MR imaging and planned follow-up lead to the diagnosis of pseudo-progression. This phenomenon has rarely been described in children with supra-tentorial low-grade gliomas after proton beam RT, particularly with this type of advanced MR technique.
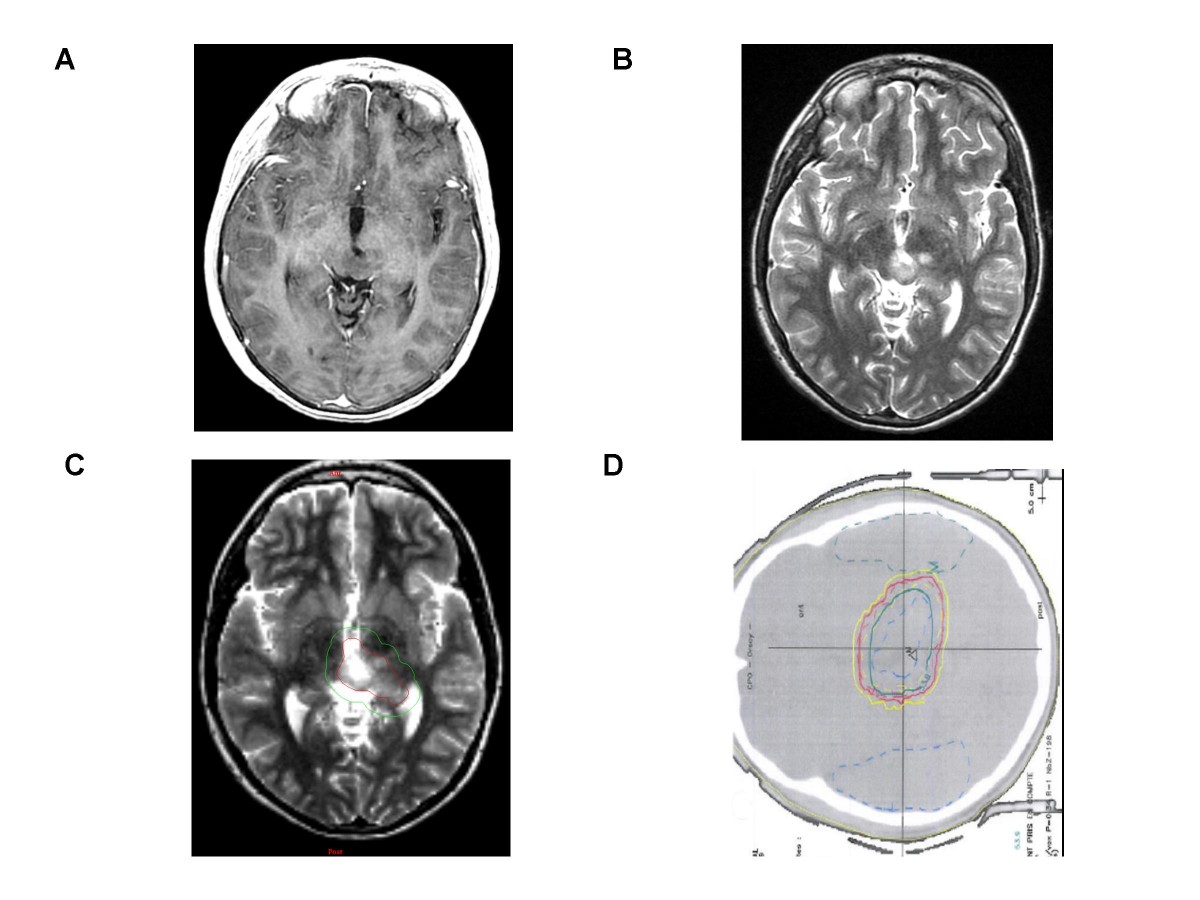
A left thalamic low-grade oligodendroglioma in a 10 year-old boy after partial resection, without contrast enhancement. [A] T1-weighted transaxial MR image after administration of intravenous Gd-DTPA [B] T2 -weighted sequence which shows ill-defined nodular images. [C] Representation of Gross tumor volume (in red) and Clinical target volume (in green). [D] Radiation field encompassing medial part of the left thalamus.
Click image to view larger.
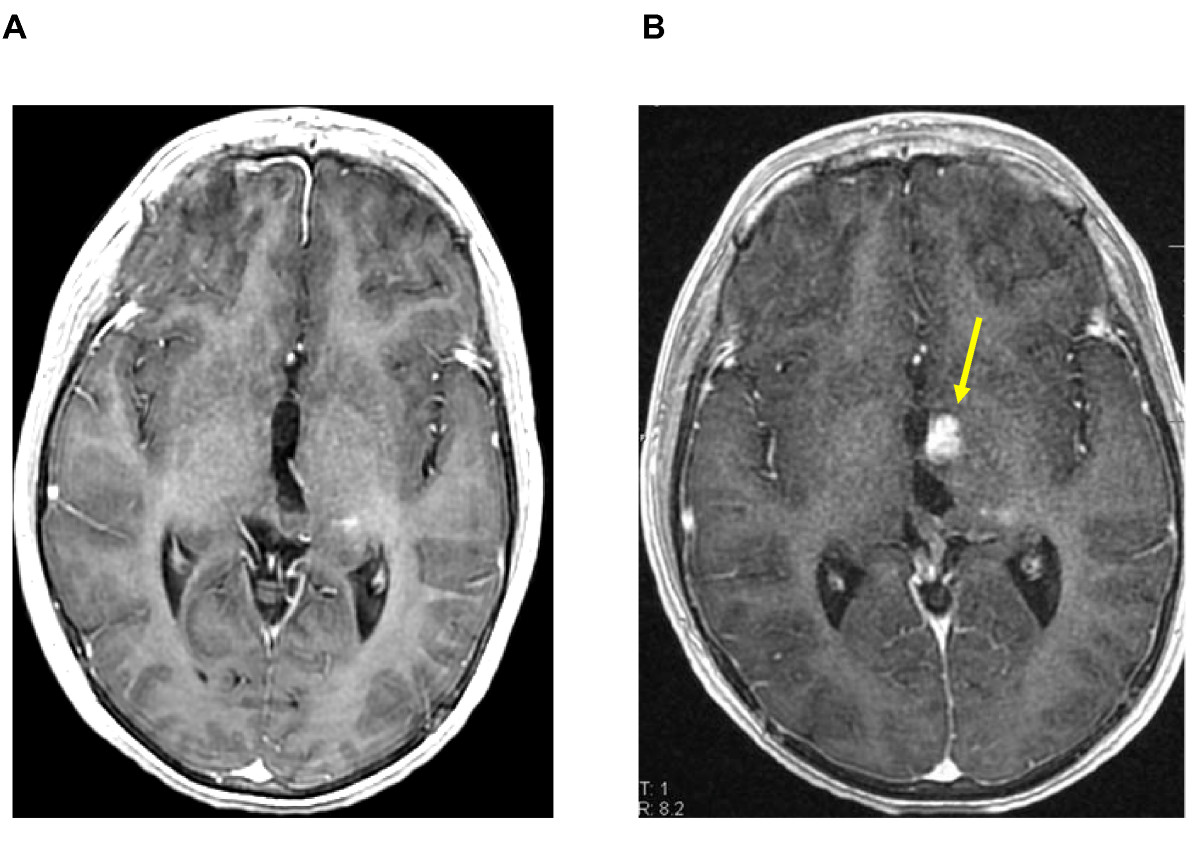
[A] T1-weighted transaxial MR image after administration of intravenous (iv) Gd-DTPA, one week before radiation. [B] The same sequence, six months after the end of irradiation (54 Gy), showing a strong contrast enhancement with a subtle mass effect (yellow arrow).
Click image to view larger.
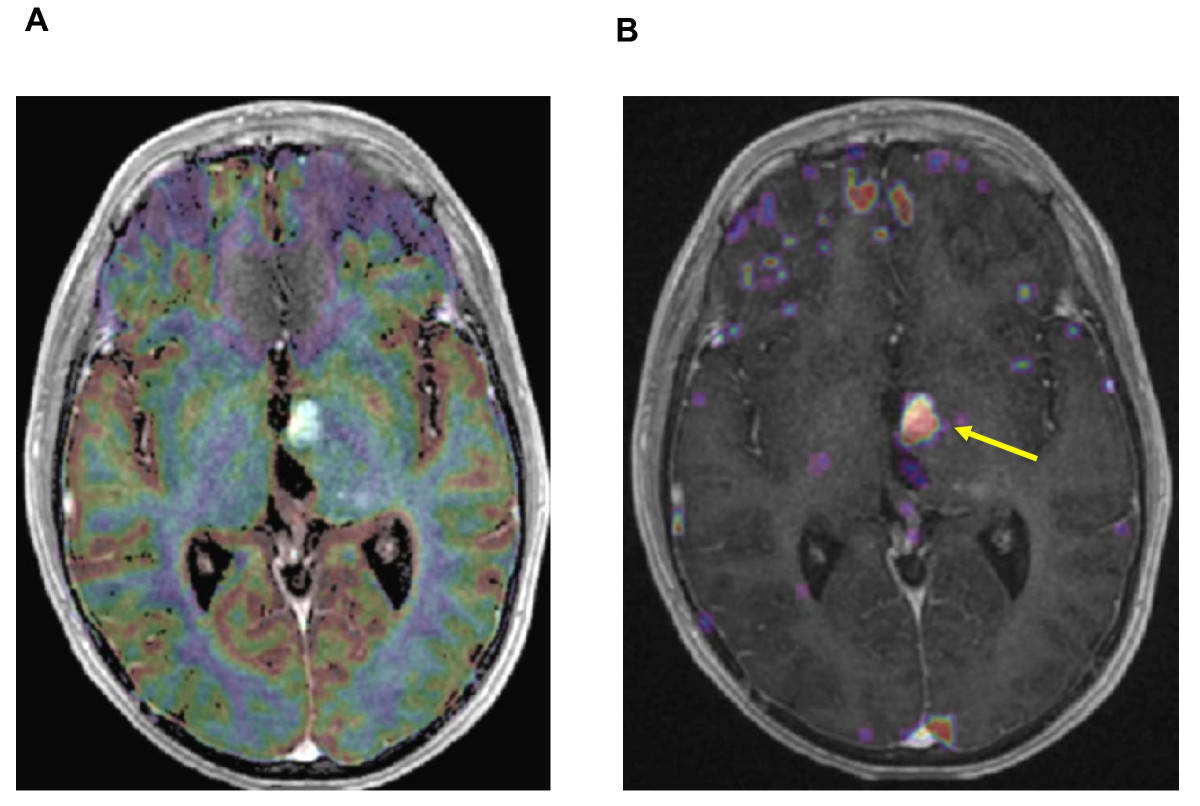
[A] Gradient-echo axial image with color overlay map showing no focus of hyperperfusion in regard of the strong contrast enhancement [B] The superimposed Permeability map with a strong microvascular leakage (yellow arrow) strictly corresponding with the enhanced area in the T1-weighted sequence.
Click image to view larger.
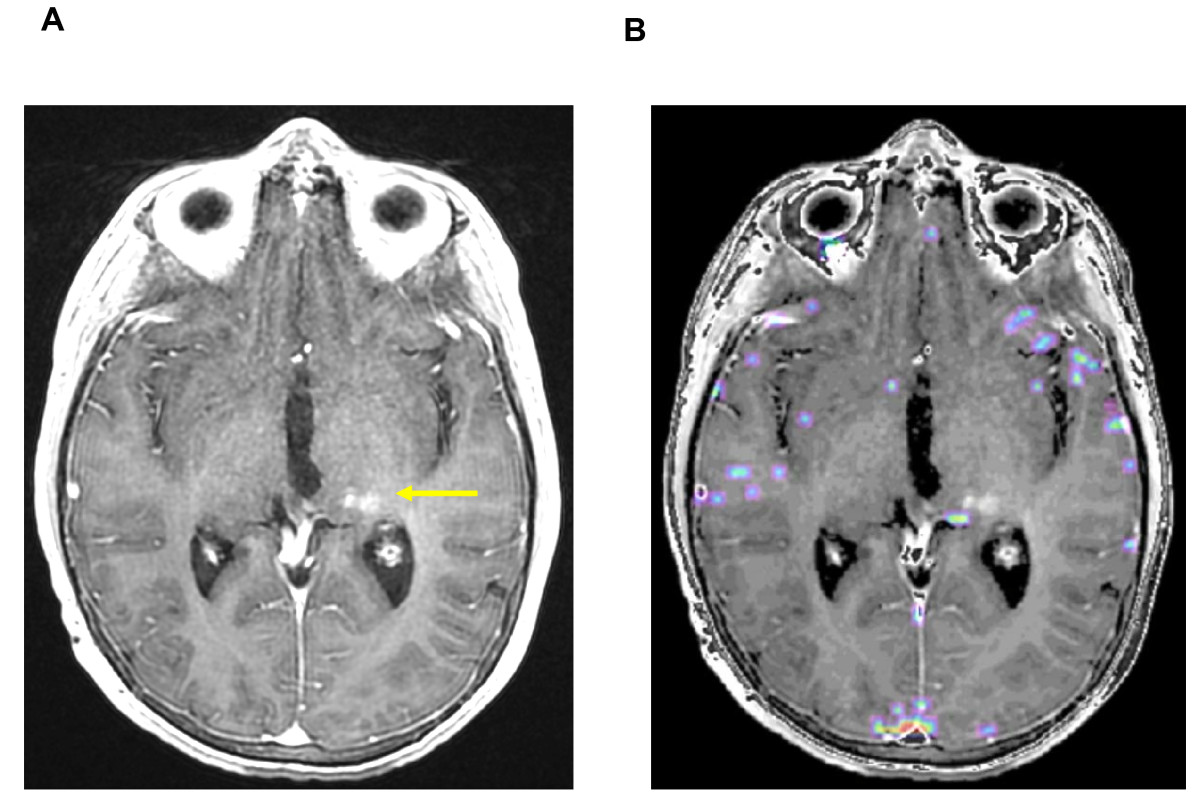
[A] T1-weighted transaxial MR image after administration of iv Gd-DTPA and [B] the superimposed Permeability map, with no contrast enhancement or detectable microvascular leakage. To be noted, a subtle hypersignal, pre-existing to the irradiation, as a post-operative modification (yellow arrow).
Click image to view larger.
The lack of typical clinical symptoms and the limits of anatomical MRI techniques imply that any subacute change suggesting disease progression may be considered as possible PsP. Post-RT therapy should not be interrupted too early(22) and DSC-MRI could help for distinguishing PsP from real progression.
Written informed consent was obtained from the parents and the patient for publication of this case report and accompagnying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
The authors declare that they have no competing interests.
CM collected the data and wrote the manuscript. FD analysed the imaging studies and contributed to the legend of figures and correction of the manuscript. DD created and developed the software used to treat T2* acquisition and produce the images. JLH supervised the irradiation of the patient. PV analysed the histology of the tumour. CSR operated the patient. CD was the treating physician of the patient. JG supervised the manuscript. All authors read and approved the final manuscript.
