
- Department of Microbiology, and Abramson Comprehensive Cancer Center, Tumor Virology Program, University of Pennsylvania, 202A Johnson Pavilion, 3610 Hamilton Walk, Philadelphia, PA 19104-6076, USA
- Pathology and Laboratory Medicine, Founders Building, 6.058 HUP/4283, 6th Floor, Philadelphia, PA 19104-6076, USA
- Botswana-University of Pennsylvania Partnership, The Children's Hospital of Philadelphia and the Center for AIDS Research, University of Pennsylvania, 3615 Civic Center Blvd, Suite 1202 ARC, Philadelphia, PA 19104-4318, USA
- University of Botswana School of Medicine PBag 0022, Gaborone
- Center for Clinical Epidemiology and Biostatistics, 832 Blockley Hall, 423 Guardian Dr. Philadelphia, PA 19104-6076, USA
- Department of Microbiology, Kochi Medical School, Kohasu, Nankoku, Kochi, 783-8505, Japan
The electronic version of this article is the complete one and can be found online at: http://www.infectagentscancer.com/content/5/1/6
Received: 6 November 2009
Accepted: 26 March 2010
Published: 26 March 2010
© 2010 Simbiri et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ocular surface squamous neoplasia (OSSN) is a rare cancer that has increased in incidence with the HIV pandemic in Africa. The underlying cause of this cancer in HIV-infected patients from Botswana is not well defined.
Tissues were obtained from 28 OSSN and 8 pterygia patients. The tissues analyzed from OSSN patients were 83% positive for EBV, 75% were HPV positive, 70% were KSHV positive, 75% were HSV-1/2 positive, and 61% were CMV positive by PCR. Tissues from pterygium patients were 88% positive for EBV, 75% were HPV positive, 50% were KSHV positive, and 60% were CMV positive. None of the patients were JC or BK positive. In situ hybridization and immunohistochemistry analyses further identified HPV, EBV, and KSHV in a subset of the tissue samples.
We identified the known oncogenic viruses HPV, KSHV, and EBV in OSSN and pterygia tissues. The presence of these tumor viruses in OSSN suggests that they may contribute to the development of this malignancy in the HIV population. Further studies are necessary to characterize the molecular mechanisms associated with viral antigens and their potential role in the development of OSSN.
Ocular surface squamous neoplasia (OSSN) is a conjunctival or corneal neoplastic growth that encompasses the conditions of simple dysplasia to conjunctival intraepithelial neoplasia (CIN) to invasive squamous cell carcinoma (1). Similar to cancer of the cervix, it has a relatively high rate of recurrence after treatment and may metastasize (2). OSSN has gained interest in the past few years in its association with the HIV pandemic and its increase in incidence is collinear with the increase in HIV (3). Prior to the HIV pandemic, OSSN was noted to occur predominantly in the elderly for whom it is the third most common oculoorbital tumor after melanoma and lymphoma (4)(5). In addition to advanced age and male sex, other risk factors linked to its pathogenesis have included ultraviolet light B rays and mutation of the p53 tumor suppressor gene (6), immunosuppression in organ transplant recipients (7), cigarette smoking, and in some settings, HPV infection (3)(8). In Africa, OSSN is becoming more common, more aggressive, and more likely to affect young people, especially females (6).
In parallel with the dramatic increase of HIV in Africa, several countries have noted a sharp rise in the incidence of OSSN in HIV infected individuals such that OSSN is currently the most common ocular tumor among adults in Africa (6)(9). Africa has the highest rate of HPV infection in the world, with an age-adjusted prevalence of 25.6% in women aged 15-74 years, followed by South America (14.3%), Asia (8.7%), and Europe (5.2%) (10). In 2006, Waddell et al. investigated the role of HIV infection in the etiology of corneo-conjunctival intraepithelial neoplasia (CIN) and carcinoma (11). The prevalence of HIV infection in these cases was 64% compared to 31% in controls (11). These findings demonstrated a strong association between increased incidence of OSSN and HIV-1 infection as applied to all tumor stages in Uganda. HIV-positive participants were markedly immunosuppressed at the time of diagnosis and their early mortality was high (11). The majority of the tumors were in the interpalpebral area of the conjunctiva, which supports the concept of UV radiation as a co-factor in the etiology of OSSN (11).
Pterygium is a raised benign growth on the eye that is most often directly related to over-exposure to the sun and dry, dusty conditions may also be a factor (12). Pterygium in the conjunctiva is characterized by elastotic degeneration of collagen and fibrovascular proliferation, and in some cases by "wing-like" conjunctival overgrowth of the cornea (13). Some studies have investigated human papillomavirus (HPV) as a risk factor for the development of pterygia (14)(15). Interestingly, recent studies have shown that pterygia can develop into OSSN, and thus may be considered a pre-malignant form of OSSN (16).
The aim of this study was to identify the viral etiologic agent(s) associated with OSSN in the HIV-infected population in Botswana. There are numerous examples of associated malignancies in the HIV population, which include CNS lymphomas with greater than 95% Epstein Barr Virus (EBV) positivity (17), pleural effusion lymphomas which are usually co-infected with both tumor gammaherpesviruses EBV and Kaposi's sarcoma associated herpes virus (KSHV) (18)(19), AIDS associated B and T cell lymphomas (20), Kaposi's sarcoma (KS)(21), Burkitt's lymphoma (BL) (22), anogenital carcinomas and papillomas (23), oral cancers (23)(24) osteosarcomas (25) mesotheliomas (25) and brain cancers (2)(18)(21)(23)(26)(27)(28). Also, the oncogenic papova virus Human papillomavirus (HPV) infects keratinocytes causing benign and malignant tumors (1). HPV proteins E6 and E7 are oncogenic and have been associated with cell immortalization and antiapoptotic effects. The HPV types 6, 11, 16, 18 and 33 have been identified in benign and malignant conjunctival lesions (3).
The role of chronic latent viruses and their intermolecular interactions in combination with other environmental factors in the context of HIV infection is likely to be important for initiating and maintaining HIV-associated malignancies. However, a causal role for these viruses is difficult to ascertain at this time. Nevertheless, infection with a range of viruses from the herspesviridae family including HSV, HCMV, EBV, and KSHV may contribute to the oncogenic process in OSSN, as has been observed with other human cancers (29).
HIV-1 infected patients with conjunctival lesions seen at Princess Marina Hospital, Gaborone, Botswana from April 11 2007 to April 14 2008 were enrolled in this study (IRB #805049 and Ministry of Health, Botswana REF NO: PPME 13/18/1 Vol III 141). Briefly, patients were identified by an ophthalmologist in the tertiary care ophthalmology clinic at Princess Marina Hospital which serves as the referral center for southern Botswana. All HIV-1 positive patients diagnosed using a HIV-ELISA (Abbott Laboratories, Hoofddorp, the Netherlands) with clinical features suggestive of OSSN or pterygium were enrolled the day before surgery. Written consent was obtained from each subject in either Setswana or English (according to subject's preference). Tissue specimens obtained in the ophthalmology operating room were divided into two pieces by the ophthalmology surgeon - one piece was sent for histopathologic analysis and the other was immediately placed in tissue transport medium for shipment to the University of Pennsylvania viral oncology laboratory. Histologic confirmation of each clinical diagnosis was obtained from the Botswana National Health Laboratory's histo- pathologist. 39 patients participated in the study, however tissue samples of varying sizes were obtained from only 36 cases. Tissues from patients included in this study were 28 whose clinical diagnosis was OSSN and 8 with pterygia (Table 1). Only patients who signed the University of Pennsylvania and Botswana Ministry of Health Institutional Review Board consent forms were included in this study. In this study all patients were enrolled from the Botswana HIV clinic. Therefore we were not able to obtain conjunctiva controls from HIV-1 negative patients or those diagnosed with OSSN and pterygia identified as HIV negative.
| Case # |
Diagnosis |
Sex |
Age |
CD4 count |
HIV Viral load |
Affected Eye |
ARV Status |
Histology Results |
| 1 |
OSSN |
M |
45 |
40 |
<400 |
Right |
+ |
SCC |
| 2 |
Pterygium |
M |
49 |
373 |
<400 |
Left |
+ |
Pterygium |
| 3 |
OSSN |
M |
39 |
64 |
<400 |
Right |
+ |
Pterygium |
| 4 |
OSSN |
M |
32 |
521 |
ND |
Right |
SCC |
|
| 5 |
OSSN |
F |
47 |
44 |
ND |
Right |
+ |
SCC |
| 6 |
OSSN |
M |
43 |
174 |
120,000 |
Right |
SCC |
|
| *7 |
Pterygium |
F |
29 |
ND |
ND |
Right |
+ |
Pterygium |
| 8 |
OSSN |
F |
42 |
134 |
120,000 |
Left |
+ |
SCC |
| 9 |
OSSN |
F |
27 |
171 |
<400 |
Left |
+ |
NA |
| *10 |
OSSN |
M |
40 |
ND |
<400 |
Right |
Severe dysplasia |
|
| 11 |
OSSN |
M |
38 |
326 |
<400 |
Left |
+ |
Severe dysplasia |
| 12 |
OSSN |
F |
22 |
457 |
ND |
- |
NA |
|
| 13 |
OSSN |
F |
44 |
ND |
<400 |
Left |
+ |
SCC |
| 14 |
OSSN |
F |
39 |
200 |
<400 |
Left |
+ |
Pterygium |
| 15 |
Pterygium |
F |
38 |
725 |
ND |
Left |
Pterygium |
|
| 16 |
Pterygium |
F |
40 |
600 |
ND |
Left |
Pterygium |
|
| 17 |
Pterygium |
F |
38 |
491 |
ND |
Left |
Pterygium |
|
| 18 |
OSSN |
F |
44 |
314 |
ND |
Left |
NA |
|
| 19 |
OSSN |
F |
37 |
56 |
<400 |
Right |
+ |
Pterygium |
| *20 |
OSSN |
M |
48 |
21 |
<400 |
Right |
+ |
SSCC |
| 21 |
OSSN |
F |
49 |
ND |
ND |
Right |
NA |
|
| 22 |
OSSN |
F |
30 |
90 |
ND |
Right |
SSCC |
|
| 23 |
OSSN |
F |
36 |
220 |
<400 |
Right |
+ |
Severe dysplasia |
| 24 |
OSSN |
F |
35 |
ND |
644,000 |
Right |
+ |
Mild dysplasia |
| 25 |
Pterygium |
F |
39 |
293 |
<400 |
Left |
+ |
Pterygium |
| 26 |
Pterygium |
M |
47 |
546 |
<400 |
Right |
Pterygium |
|
| 27 |
Pterygium |
F |
31 |
113 |
ND |
Left |
+ |
Pterygium |
| 28 |
OSSN |
M |
50 |
87 |
<400 |
Right |
+ |
SCC |
| 29 |
OSSN |
F |
34 |
192 |
ND |
Left |
SCC |
|
| 30 |
Pterygium |
F |
29 |
70 |
<400 |
Right |
+ |
Pterygium |
| 31 |
OSSN |
M |
45 |
62 |
17,000 |
Left |
+ |
NA |
| 32 |
OSSN |
F |
28 |
107 |
<400 |
Left |
+ |
Severe dysplasia |
| 33 |
OSSN |
F |
42 |
236 |
342 |
Left |
Pterygium |
|
| 34 |
OSSN |
M |
33 |
94 |
81,972 |
Left |
+ |
SCC |
| 35 |
OSSN |
M |
40 |
64 |
685,000 |
Right |
+ |
Cancer in situ |
| 36 |
OSSN |
F |
36 |
38 |
200,000 |
Right |
+ |
NA |
| 37 |
OSSN |
F |
49 |
ND |
ND |
Right |
Severe dysplasia |
|
| 38 |
OSSN |
F |
24 |
31 |
ND |
Left |
+ |
Moderate dysplasia |
| 39 |
OSSN |
F |
44 |
121 |
ND |
Right |
SCC |
* Tissue not available, NA - Not available
The table shows patient diagnosis, sex, age on entering study, CD4 counts, viral load, the eye affected, the retroviral therapy status of each patient, and histology results. Tissues were not obtained from 3 patients and indicated with an asterisk. Patients #s 3, 14, 19, and 33 were diagnosed as OSSN but histology results indicated that they were pterygia.
Simbiri et al. Infectious Agents and Cancer 2010 5:6 doi:10.1186/1750-9378-5-6
PCR analysis was performed as previously described [31-35] with each virus specific primer (see Figure 1C).
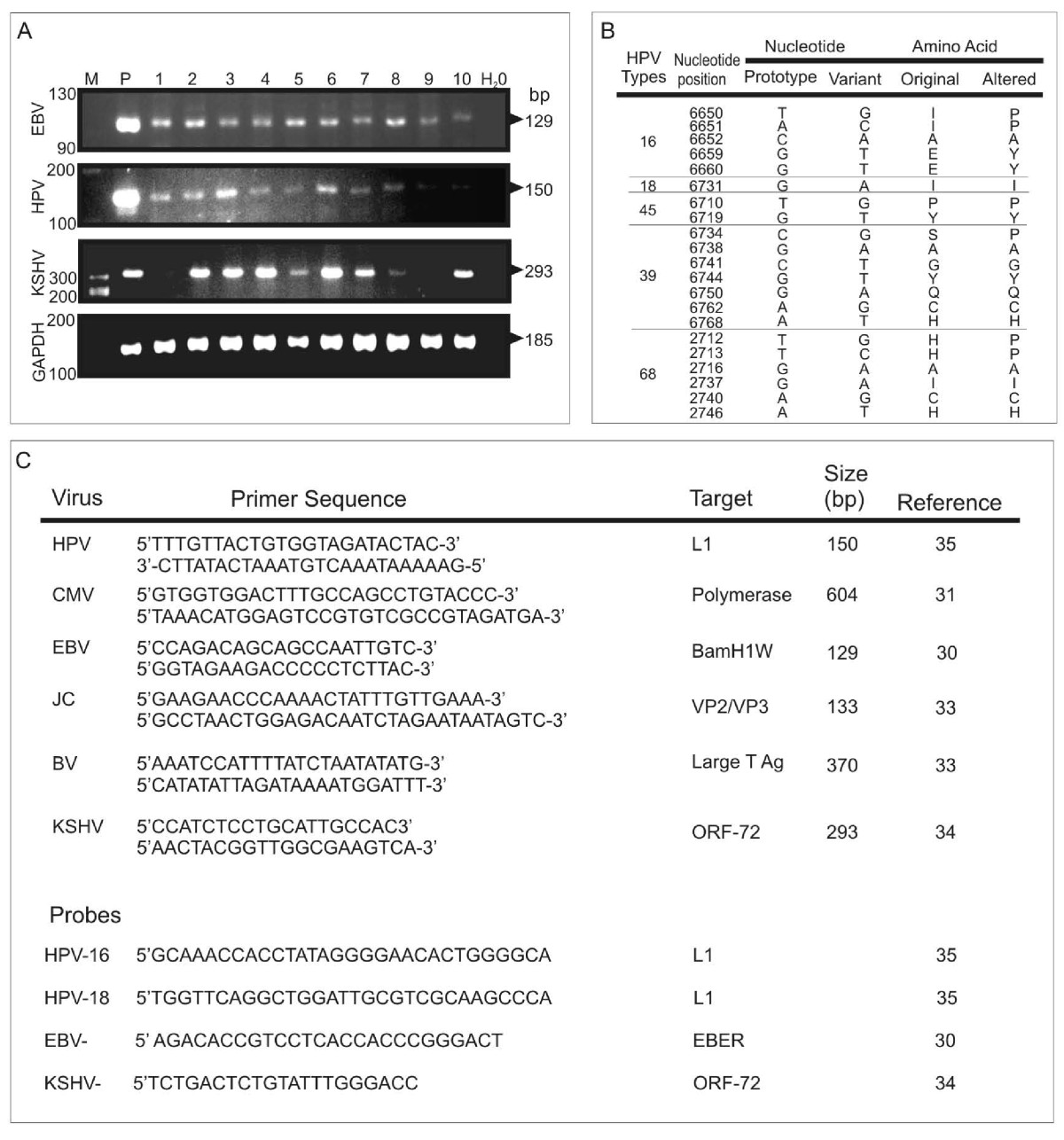
A. Representative PCR analysis of tumor virus detection from OSSN tumor samples. For EBV PCR, LCL-2 105 cells which contain 20-50 copies of EBV per genome were used as positive control and distilled water as control for PCR mix. For HPV, Hela 105 cells which contain 10-20 copies of HPV-18 per genome were used as positive control and distilled water as control for PCR mix. Similarly for KSHV we used BCBL1 cells which contain 30-50 copies of KSHV per genome as positive control and distilled water as control for PCR mix. The PCR products are shown after electrophoresis on a 3% agarose gel containing 100 ng/ml ethidium bromide. PCR product size for each virus type is shown on the right side. We show representative gels showing the PCR results of which EBV was detected in 83% of the samples, HPV in 75% of the samples, KSHV in 70% of the samples and CMV in 61% of the samples. We did not detect JC and BK virus in any sample. B. Representative point mutations in HPV-L1 nucleotide and amino acid sequence variation in OSSN biopsies. We detected HPV-16, 18, 45, 39, and 68 isolates. As shown, the changes were mainly missense and nonsense mutations. C. Shows the primer sequences used in the PCR analysis of the oncogenic viruses in OSSN and pterygia tissues and probes used for in situ hybridization.
Click image to view larger.
To support our PCR findings for the presence of HPV, EBV, and KSHV in tissues we performed in situ hybridization and immunohistochemistry on 5 μm thick paraffin-embedded sections to detect virus specific antigens. We noted alignment with the probes for HPV-16-L1 at 481-511 bp (accession DQ155283), EBV-EBER at 1-26 bp (accession J02078) and for KSHV-ORF-72 at 201-220 bp (accession 009333). In situ hybridization probes for HPV-16 or 18 (36), EBV-EBER (30), and KSHV-ORF-72 (34) were labeled with digoxigenin-ddUTP (Dig) using a commercial kit (Roche Inc., Indianapolis, IN) and used as described previously (37). We used commercial antibodies HPV 16-L1 and HPV 18-E6 (DAKO Inc., Carpentaria, CA), and monoclonal antibody S12 for EBV-LMP1, and monoclonal antibody derived from KSHV encoded LANA for immunohistochemistry (38). Results from the ISH and IHC were analyzed by a licensed histopathologist at the University of Pennsylvania, School of Medicine.
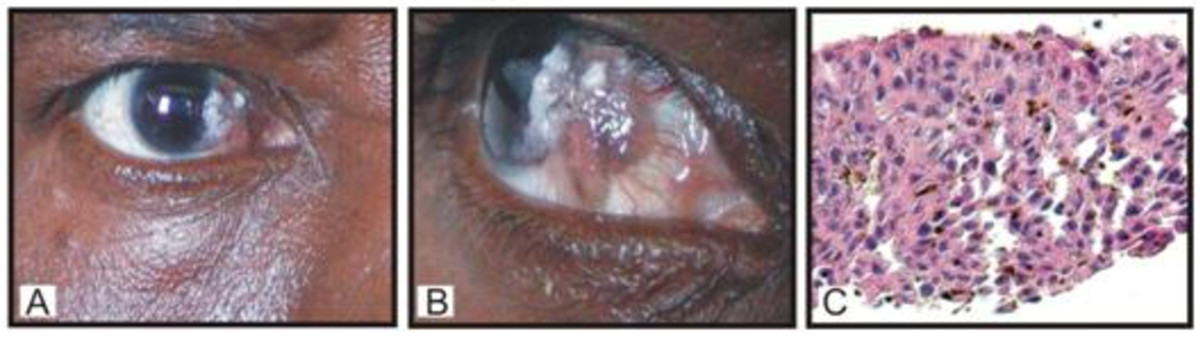
H&E staining showing features of in situ carcinoma characterized by full thickness changes in nuclear: cytoplasm ratio, nuclear pleomorphism, dyskeratotic cells, and presence of koilocytes.
Click image to view larger.
| Case # |
Diagnosis |
HPV |
EBV |
KSHV |
CMV |
BK |
JC |
HSV 1/2 |
| 1 |
OSSN |
+ |
+ |
- |
- |
- |
- |
+ |
| 2 |
Pterygium |
+ |
+ |
+ |
+ |
- |
- |
+ |
| 3 |
OSSN |
+ |
+ |
+ |
+ |
- |
- |
+ |
| 4 |
OSSN |
+ |
+ |
+ |
- |
- |
- |
+ |
| 5 |
OSSN |
+ |
+ |
- |
+ |
- |
- |
+ |
| 6 |
OSSN |
+ |
+ |
+ |
+ |
- |
- |
+ |
| 8 |
OSSN |
+ |
+ |
+ |
- |
- |
- |
+ |
| 9 |
OSSN |
+ |
+ |
- |
- |
- |
- |
+ |
| 11 |
OSSN |
+ |
+ |
+ |
- |
- |
- |
- |
| 12 |
OSSN |
+ |
+ |
+ |
- |
- |
- |
- |
| 13 |
OSSN |
-/+ |
+ |
- |
+ |
- |
- |
- |
| 14 |
OSSN |
- |
- |
+ |
+ |
- |
- |
+ |
| 15 |
Pterygium |
- |
+ |
+ |
+ |
- |
- |
+ |
| 16 |
Pterygium |
- |
+ |
- |
+ |
- |
- |
+ |
| 17 |
Pterygium |
- |
+ |
+ |
- |
- |
- |
+ |
| 18 |
OSSN |
- |
+ |
+ |
+ |
- |
- |
+ |
| 19 |
OSSN |
- |
+ |
+ |
- |
- |
- |
- |
| 21 |
OSSN |
- |
+ |
+ |
- |
- |
- |
- |
| 22 |
OSSN |
- |
+ |
- |
- |
- |
- |
- |
| 23 |
OSSN |
- |
+ |
+ |
+ |
- |
- |
+ |
| 24 |
OSSN |
- |
+ |
+ |
+ |
- |
- |
- |
| 25 |
Pterygium |
- |
+ |
- |
+ |
- |
- |
+ |
| 26 |
Pterygium |
+ |
- |
+ |
+ |
- |
- |
- |
| 27 |
Pterygium |
+ |
+ |
+ |
- |
- |
- |
+ |
| 28 |
OSSN |
+ |
+ |
- |
- |
- |
- |
+ |
| 29 |
OSSN |
+ |
- |
+ |
+ |
- |
- |
+ |
| 30 |
Pterygium |
+ |
+ |
- |
+ |
- |
- |
- |
| 31 |
OSSN |
+ |
+ |
+ |
+ |
- |
- |
+ |
| 32 |
OSSN |
- |
+ |
- |
+ |
- |
- |
+ |
| 33 |
OSSN |
+ |
- |
+ |
+ |
- |
- |
+ |
| 34 |
OSSN |
+ |
+ |
+ |
- |
- |
- |
- |
| 35 |
OSSN |
+ |
- |
+ |
- |
- |
- |
- |
| 36 |
OSSN |
+ |
+ |
- |
+ |
- |
- |
+ |
| 37 |
OSSN |
+ |
- |
+ |
+ |
- |
- |
+ |
| 38 |
OSSN |
+ |
+ |
+ |
+ |
- |
- |
+ |
| 39 |
OSSN |
+ |
+ |
+ |
+ |
- |
- |
+ |
Oncogenic viruses identified in each OSSN and pterygium patient as determined by PCR analysis. Most cases tested positive for HPV, EBV, KSHV, and HSV. HPV results for samples 14-24 were intriguing since most were positive on IHC and ISH. None was positive for BK and JC.
Simbiri et al. Infectious Agents and Cancer 2010 5:6 doi:10.1186/1750-9378-5-6
| Virus Type |
OSSN |
Pterygium |
|---|---|---|
| HPV-6 |
21% |
0 |
| HPV-11 |
46% |
63% |
| HPV-16 |
61% |
75% |
| HPV-18 |
54% |
63% |
| HPV-31 |
25% |
0 |
| HPV-33 |
4% |
0 |
Proportion of HPV types identified in patient samples by use of type specific HPV primers, HPV types 6, 11, 16, 18, 31, and 33. It is noted that HPV-11, 16, and 18 were common in both OSSN and pterygia cases, with HPV-6, 31, and 33 only detected in OSSN cases.
Simbiri et al. Infectious Agents and Cancer 2010 5:6 doi:10.1186/1750-9378-5-6
| Case # |
Diagnosis |
HPV |
EBV |
KSHV |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IHC |
ISH |
PCR |
IHC |
ISH |
PCR |
IHC |
ISH |
PCR |
||
| 1 |
OSSN |
- |
- |
+ |
+ |
+ |
+ |
+ |
+ |
- |
| 2 |
Pterygium |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 3 |
OSSN |
+ |
+ |
+ |
+ |
- |
+ |
+ |
- |
+ |
| 4 |
OSSN |
+ |
- |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 5 |
OSSN |
+ |
+ |
+ |
- |
+ |
+ |
+ |
+ |
- |
| 6 |
OSSN |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 8 |
OSSN |
+ |
+ |
+ |
+/- |
+/- |
+ |
- |
- |
+ |
| 9 |
OSSN |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
- |
| 11 |
OSSN |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 12 |
OSSN |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 13 |
OSSN |
-/+ |
-/+ |
-/+ |
+ |
- |
+ |
+ |
+ |
- |
| 14 |
OSSN |
+ |
+ |
- |
+ |
+ |
- |
+ |
- |
+ |
| 15 |
Pterygium |
+ |
+ |
- |
+ |
+ |
+ |
+ |
+ |
+ |
| 16 |
Pterygium |
+ |
+ |
- |
+ |
- |
+ |
+ |
+ |
- |
| 17 |
Pterygium |
+ |
- |
- |
+ |
+ |
+ |
+ |
+/- |
+ |
| 18 |
OSSN |
+ |
+ |
- |
+ |
+ |
+ |
+ |
+ |
+ |
| 19 |
OSSN |
+ |
+ |
- |
+ |
+ |
+ |
+ |
+ |
+ |
| 21 |
OSSN |
+ |
+ |
- |
+ |
+ |
+ |
+ |
+ |
+ |
| 22 |
OSSN |
+ |
+ |
- |
+ |
+ |
+ |
+ |
+ |
- |
| 23 |
OSSN |
+ |
- |
- |
+ |
+ |
+ |
+ |
+/- |
+ |
| 24 |
OSSN |
+ |
+ |
- |
+ |
+ |
+ |
+ |
+ |
+ |
| 25 |
Pterygium |
+ |
+/- |
- |
+ |
+ |
+ |
+ |
+ |
- |
| 26 |
Pterygium |
+ |
+ |
+ |
+ |
+ |
- |
+ |
- |
+ |
| 27 |
Pterygium |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 28 |
OSSN |
+ |
+/- |
+ |
+ |
+ |
+ |
+ |
+ |
- |
| 29 |
OSSN |
+ |
+ |
+ |
+ |
+ |
- |
+ |
+ |
+ |
| 30 |
Pterygium |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
- |
| 31 |
OSSN |
+ |
+ |
+ |
- |
- |
+ |
+/- |
+/- |
+ |
| 32 |
OSSN |
- |
- |
- |
+ |
+ |
+ |
+ |
+ |
- |
| 33 |
OSSN |
+ |
- |
+ |
+ |
+ |
- |
+ |
- |
+ |
| 34 |
OSSN |
- |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 35 |
OSSN |
+ |
+ |
+ |
+ |
+ |
- |
+ |
+ |
+ |
| 36 |
OSSN |
+ |
+ |
+ |
+ |
- |
+ |
+ |
+ |
- |
| 37 |
OSSN |
- |
- |
+ |
+ |
+ |
- |
+ |
+ |
+ |
| 38 |
OSSN |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| 39 |
OSSN |
+ |
+ |
+ |
- |
- |
+ |
+ |
+ |
+ |
+/- Indeterminate
Oncogenic viruses identified in each patient by Immunohistochemistry and In situ hybridization. It is noted that for each of the samples analyzed for the specific viruses-HPV-16/18, EBV, and KSHV, there was high concordance in IHC and ISH. For each virus a column for PCR results has been added for comparison. Due to lack of specimen we were unable to test for the other viruses. No tissue samples were available for patients 7, 10, and 20.
Simbiri et al. Infectious Agents and Cancer 2010 5:6 doi:10.1186/1750-9378-5-6

Panels A-C shows results from Sense probe negative controls with no detectable nuclear staining. Panels D-F the positive cells of tissue sections probed with HPV-L1, EBV-EBER, and KSHV-ORF72 showed dark brown staining of the nucleus. The probes did not detect all viruses in all tumor cells, however, HPV, EBV, and KSHV were detected in some regions. Panels G-I shows a higher magnification of 60× compared to panels D-F which showed magnification of 40×.
Click image to view larger.
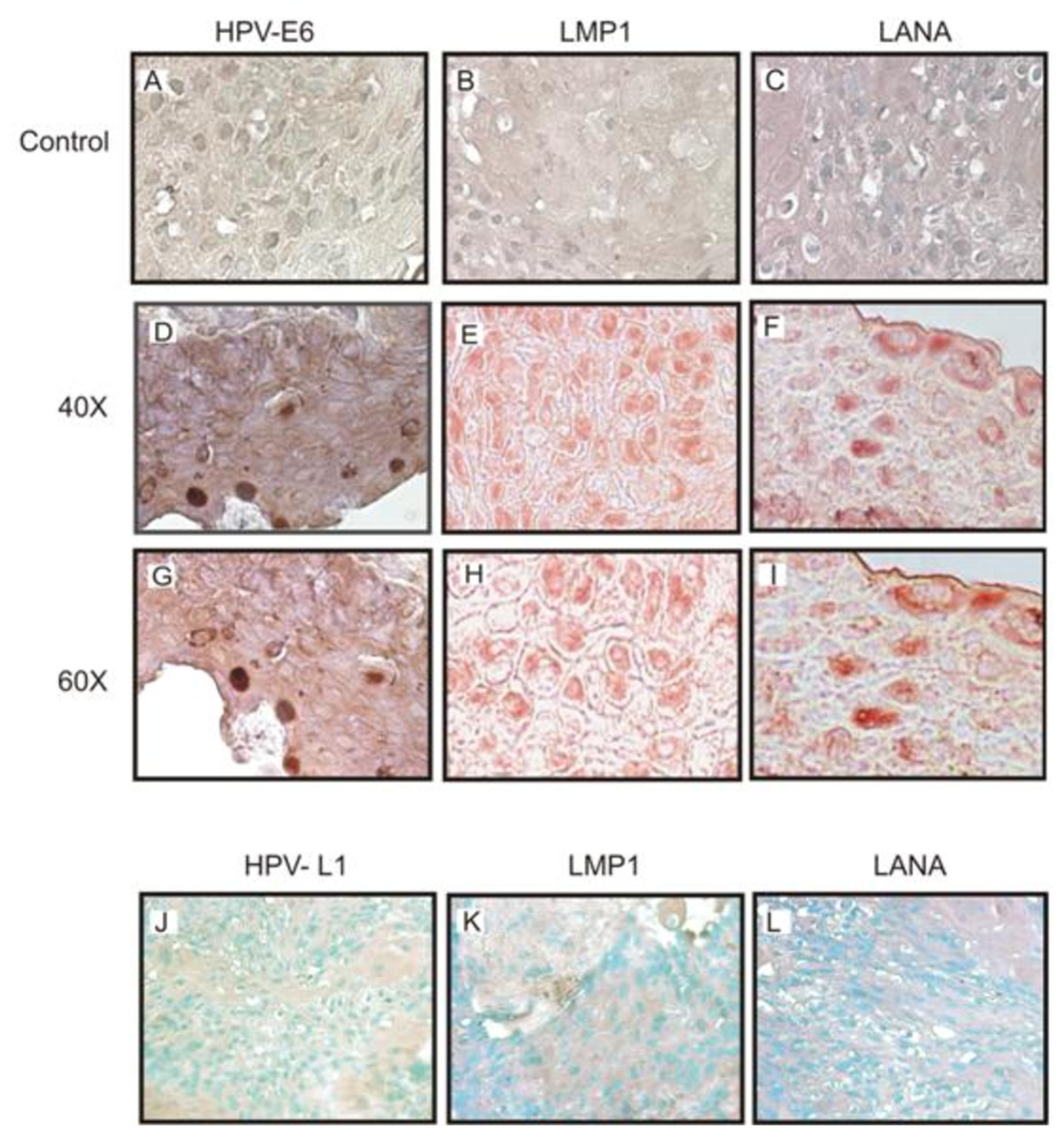
Panels A-C shows no nuclear staining in the negative controls, Panels D-F show positive cells as dark brown staining of the nucleus with HPV-E6 antibody, as well as positive staining for LMP1 and LANA using EBV-LMP1 hybridoma supernatant and KSHV-LANA specific antibody. Panels G-I shows a higher magnification of 60× compared to panels D-F taken at 40×. Panels J-L are immunohistochemistry results for negative samples showing no detectable staining which would represent positive signals.
Click image to view larger.
| Case # |
HPV type |
|---|---|
| 1 |
7,13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 2 |
7,13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 3 |
7,13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 4 |
7,13,16,18,39,40,43,59,61,68,70,77,91,97 |
| 5 |
7,13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 6 |
7,13,16,18,39,40,43,59,68,70,77,91,97 |
| 8 |
7,13,16,18,29,39,40,43,45,59,61,68,70,77,85,91,97 |
| 9 |
7,13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 11 |
7,13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 12 |
16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 13 |
7,13,16,18,39,40,43,45,59,61,68,70,74,85,91,97 |
| 14 |
16,18,29,39,40,43,45,59,68,70,85,91,97 |
| 15 |
7,13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 16 |
7,13,16,18,39,40,43,45,59,61,68,70,74,77,85,91,97 |
| 17 |
7,13,16,18,29,39,40,43,45,59,61,68,70,77,85,91,97 |
| 18 |
7,16,18,39,40,61,70,77,85,91,97 |
| 19 |
16,18,39,40,43,45,61,70,77,85,91,97 |
| 21 |
7,13,16,40,45,70,77,85 |
| 22 |
7,13,16,39,43,45,70,85 |
| 23 |
7,13,43,45,70,77,85 |
| 24 |
7,43,45,85 |
| 25 |
13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 26 |
13,16,18,39,40,43,45,59,61,68,70,77,85,91,97 |
| 27 |
1,3,7,11,13,16,18,39,40,43,45,59,61,68,70,77,85,89,91,97 |
| 28 |
29,43,45,59,85 |
| 29 |
45,59,68,70,85 |
| 30 |
1,3,7,11,13,16,18,39,40,43,45,59,61,68,70,77,85,89,91,97 |
| 31 |
16,18,43,45,59,68,70 |
| 32 |
16,18,43,45,59,61,68,70 |
| 33 |
1,13,16,18,39,40,43,44,45,55,59,61,68 |
| 34 |
7,13,16,18,39,43,45,59,61,68,97 |
| 35 |
7,16,18,39,40,43,45,59,61,68,74 |
| 36 |
16,18,39,45,59,61,68,77,97 |
| 37 |
7,13,16,18,39,43,45,59,61,68,77,97 |
| 38 |
7,13,16,18,39,40,43,44,45,55,59,68,74,77,97 |
| 39 |
7,18,39,40,43,59,61,68,74,77,91,97 |
HPV types identified in patient samples by sequencing with the consensus primer GP5+/GP6+. The most commonly identified HPV type in both OSSN and pterygium tissues included the high risk HPV-18, 16, 45, 39, 59, and 68.
Simbiri et al. Infectious Agents and Cancer 2010 5:6 doi:10.1186/1750-9378-5-6
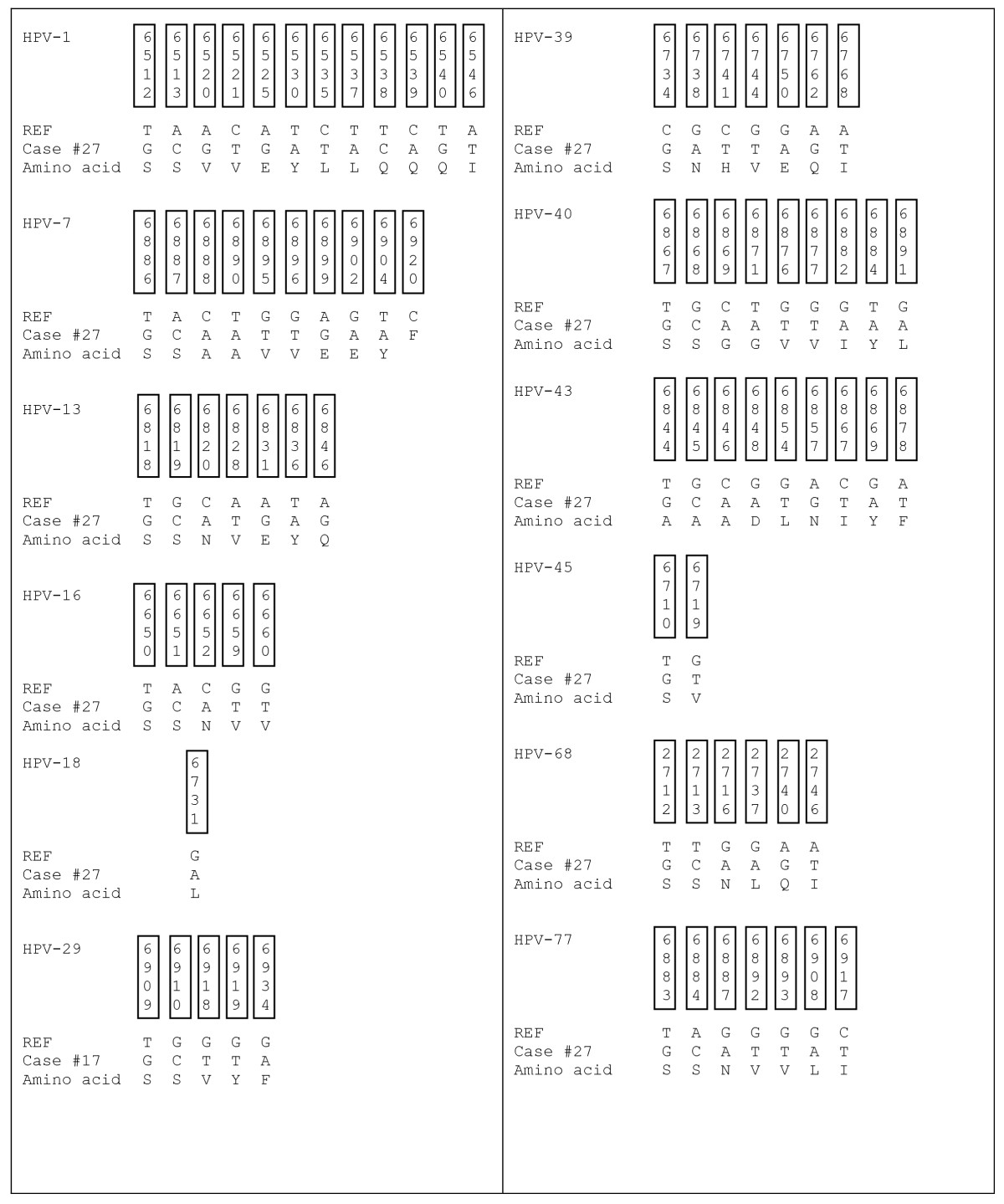
Shown are representative samples of the most common HPV types detected by sequencing using GP5+/GP6+ primers of the L1 region. The table shows nucleotide variation and amino acid changes. The top 4 rows show the nucleotide position, the 5th row shows the HPV reference nucleotide sequence, the 6th row shows the variation in patient nucleotide sequence, and the 7th row is the resulting variant amino acid sequence. In each HPV type, the variations were the same for each study case in the selected nucleotide sequence with some differences upstream and downstream in the different subjects, except case #15 which varied in a specific nucleotide in all HPV types, besides HPV-1.
Click image to view larger.
A dramatic increase in OSSN has been noted in sub-Saharan Africa over the last 10 years in HIV population (1). In Uganda there has been an increase in incidence especially among young people linked to HIV infection (6). In Botswana, data from Princess Marina Hospital in Gaborone currently indicates a pronounced increase in incidence of OSSN in young HIV-1 infected individuals. This initial study concurrently detected the presence of multiple tumor viruses in OSSN tissues. For the first time we showed the presence of HPV, EBV, KSHV, and CMV in ocular tissues in HIV/AIDS patients. Association of viruses with human cancers have already been reported, such as KSHV with KS and PEL (41), EBV with primary CNS lymphoma (17), nasopharyngeal carcinoma (26), and Burkitt's lymphoma (22), HPV with cervical cancer (2), anal cancer (42), and testicular cancer (43), However, the level of contribution by HIV to the development of human malignancies remains unclear and is likely to be through several mechanisms.
Infection and establishment of latency are mediated by viral proteins expressed in infected cells. Importantly, the immunomodulatory mechanisms used by one virus may actually enhance or benefit the activity or replication of other viruses. Many of these viruses (for example, HPV, CMV, and EBV) are quite common in the human population (44), but do not always lead to development of malignancies in healthy individuals with a competent immune system. However, infection with HIV resulting in immunosuppression may eventually tip the balance in favor of the tumor viruses, leading to an increased risk of cancer in the immune compromised individuals. The localization of these oncogenic proteins in the OSSN tissues show association, however establishment of a causal effect by any of the viruses, or a multiple of the viruses in an HIV atmosphere has yet to be fully confirmed. Determining the pathways involved in the initiation and establishment of the cancers in HIV patients compared to non-HIV patients will give us a better understanding of the interplay of the different oncogenic viral proteins within the normal immune system and immunosuppressed system. Though we have shown the presence of these viral proteins in the OSSN tissue, some investigators have not identified viral sequences in squamous cell conjunctival carcinoma (SCCC) which has also increased in the HIV infected population and has been suspected of having viral etiology (45)(46). Therefore, more studies are clearly needed to fully establish a role for these viruses in OSSN.
The localization of different tumor viruses in similar tissue sections suggest that these viruses may functionally interact to contribute to the OSSN phenotype. Similar to our findings of HPV and EBV in ocular tissues, Prayitno reported that in 19 cervical carcinoma samples 89% were positive for HPV and 68% were positive for EBV (47). Nakamura et al suggested that HPV probably does not act alone in initiating ocular neoplasia, but that other factors including the ultraviolet light were involved (37). Whereas studies involving HPV and cervical cancer have been associated with oncogenic HPV-16 and 18, our study identified HPV-6, 7,16, 18, 31, 45, and 97 in DNA from the OSSN and pterygia tissues as determined by PCR. Interestingly, we detected nucleotide sequences from HPV-1, 3, 7, 13, 16, 18, 29, 31, 33, 39, 40, 43, 44, 45, 55, 59, 61, 68, 70, 74, 77, 85, 89 91, and 97 by sequencing PCR amplicons from the different tissues. Some of the sequence alignments had scores greater than 80% with specific HPV types indicating presence of these HPV types or their variants in some of the samples. This suggests exposure to many types of HPV in this population, some of which are oncogenic, which with other factors may trigger cell proliferation leading to OSSN and other cancers in the immunocompromised patients. The selection pressure that may exist as a consequence of competition between opportunistic infections may further lead to mutations occurring in the HPV types as well as the other infectious agents. Interestingly, there was a significant amount of amino acid variation within the cases to suggest different HPV types when each sequence was aligned with the specific HPV prototype.
To corroborate the PCR results we performed in situ hybridization and immunohistochemistry studies. These results showed that in the invasive OSSN tissues the viruses were localized in similar tissue sections. Some of the viral genomes are likely to be integrated by their punctate signals and episomal viral DNA by their diffuse signal throughout the nucleus (24). The number of cells positive for viral signals were modest, possibly a factor of the limited size of tissues tested, relatively small size of the tissue obtained for analysis, and lower sensitivity compared to PCR. Previous reports have suggested that infection with more than one HPV type enhances cervical cancer and oral squamous carcinoma (23). Also, Mirzamani et al reported co-infections with EBV and HPV-16/18 in nasopharyngeal carcinoma (NPC) patients and concluded that both viruses were important in contributing to the pathogenesis of NPC (26). It is not known if cases with OSSN without HIV infection had similar outcome with HPV and other viruses as we were unable to obtain these tissue samples. Moubayed et al reported HPV-6/11, HPV-16, and HPV-18 in a Tanzanian study, with the conclusion that it was HPV-16 and HPV-18 that was associated with OSSN (48). They noted that the intensity of in situ hybridization was highly variable ranging from barely detectable to a few grains over some cells located near the surface of the lesions (48). As in some of our hybridization results they noted nuclear or perinuclear staining within the epithelial lesions and a complete absence of hybridization signals in the subepithelial layers and the surrounding unaffected epithelium.
The significance of all the HPV types identified with respect to OSSN oncogenesis in individual patients, and specifically the infection with multiple oncogenic HPV types-both high risk and low risk, EBV, and KSHV viruses requires careful examination. Some studies have indicated that the oncogenic capacity of HPV variants may also differ between geographic regions based on HLA allele distribution in these populations (40). The unknown impact of HLA allele differences, HPV variants, and other oncogenic viruses in this HIV-1 infected population is of significance and warrants further investigation.
In tropical countries secondary immunodeficiency attributable to chronic inflammation caused by parasitic or viral infections might contribute to tumorigenesis. The high frequency of coinfection of HPV, EBV, KSHV, CMV, and HIV in the OSSN patients may be a result of cooperative and complementary interactions of the viruses. In addition, we suggest that the disease might be more aggressive in HIV patients due to their immune dysfunction, abnormal cytokine and chemokine expression, growth factor production and exposure to ultraviolet rays. In this sample we cannot determine if the patients were initially infected with HPV, or HIV and other oncogenic viruses before occurrence of OSSN, or if some of the viruses were opportunistic infections as a result of OSSN disease or HIV infection. The effect of latency in ubiquitous viruses like EBV, HPV and high prevalence of sexually transmitted HSV and KSHV is not clear in this OSSN population. It has been reported, and we also note that the course of OSSN is more rapid in HIV infected patients and the occurrence is increasing in younger patients with HIV at a higher rate (3)(6). In HIV infected patients, it is not known at what stage OSSN occurs. Spitzer et al in a Malawi study reported that OSSN was the first detectable sign of HIV infection in the majority of cases (7).
This study investigating the link between oncogenic viruses in OSSN in the HIV population suggests that multiple viral agents may have a role in development of this disease. The interaction between different viral antigens and their regulatory activities in immunocompromised individuals will contribute to cell survival and proliferation in the infected cells. Clearly, further study is warranted to understand the molecular processes involved in the increased incidence of OSSN in the HIV population.
